 by Daniel P. Friedmann, MD, FAAD; Vineet Mishra, MD, FAAD; and Trevor Batty, BS
by Daniel P. Friedmann, MD, FAAD; Vineet Mishra, MD, FAAD; and Trevor Batty, BS
Dr. Friedmann is with the Westlake Dermatology Clinical Research Center at Westlake Dermatology & Cosmetic Surgery in Austin, Texas. Dr. Mishra is with the Division of Dermatology and Cutaneous Surgery at the University of Texas Health Science Center at San Antonio in San Antonio, Texas. Mr. Batty is with the Arizona College of Osteopathic Medicine at Midwestern University in Glendale, Arizona.
Funding: No funding was provided.
Disclosures: The authors have no conflicts of interest relevant to the content of this article.
Abstract: This case report highlights a unique variant of seborrheic dermatitis (SD) in a 30-year-old African-American woman with progressive facial papules. Four weeks of uninterrupted mild potency topical corticosteroid therapy produced marked improvement of signs and symptoms of biopsy-confirmed SD. SD mimicking cutaneous sarcoidosis is a unique treatment-responsive variant of SD that may be more likely to be encountered in African-American patients.
Keywords: Seborrheic dermatitis, malassezia, facial papules, topical corticosteroid, cutaneous sarcoidosis
J Clin Aesthet Dermatol. 2018;11(7):44–45
Introduction
Seborrheic dermatitis (SD) is a common dermatologic disorder with a prevalence of approximately five percent, most often seen in young adult and elderly men.1 Patients typically present with symmetrical, well-demarcated red patches and plaques with overlying yellow greasy scale and potential symptoms of burning and pruritus. Distribution is most common in areas rich in sebaceous glands such as the scalp, eyebrows, and glabella.2 A petaloid variant of SD is not uncommon in African-American patients, presenting as scaly, polycyclic coalescing rings in characteristic areas of the face and chest. We present a case of a uniquie variant of SD in a young adult African-American woman, who presented with progressive facial papules.
Case Vignette
A 30-year-old African-American woman presented with a three-year history of a progressively worsening rash on her face, characterized by dark-colored lesions with periodic background scaling, burning, and pruritus. She was previously treated with an unspecified shampoo and topical product prescribed by an outside dermatologist without significant improvement. The patient had a history of hypothyroidism, asthma, mild eczema, and severe environmental allergies.
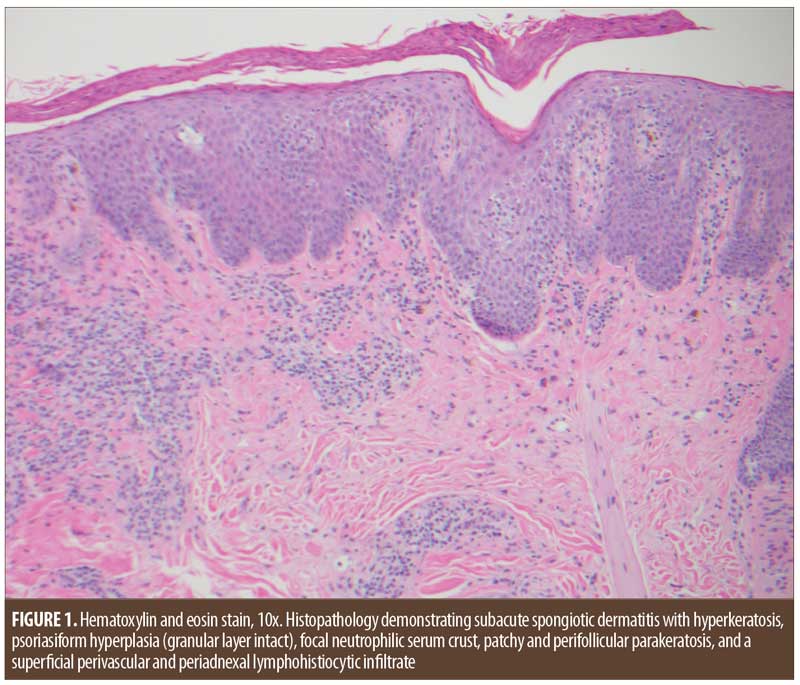
Physical examination revealed hyperpigmented, flattened granulomatous papules, at times confluent into plaques, and mild background scaling located on the temples, lateral malar cheeks, and nasal ali bilaterally. Minimal to no scaling or erythema was present in the scalp, perinasal grooves, or nasolabial folds. A punch biopsy was obtained from the left malar cheek and histopathologic features were consistent with seborrheic dermatitis (Figure 1).
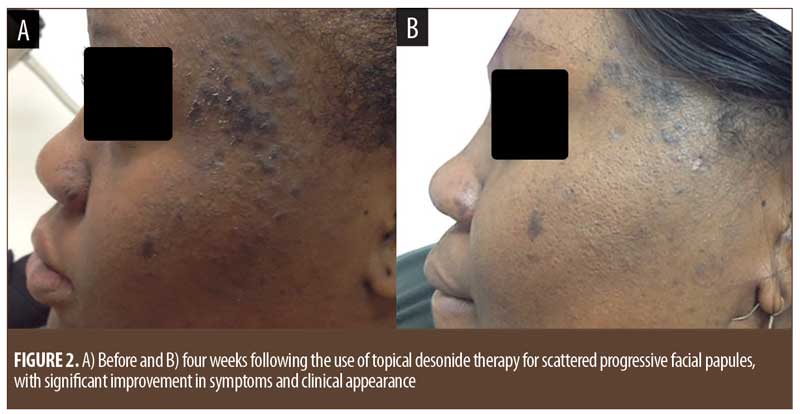
A regimen of topical desonide 0.05% cream twice daily to affected areas and zinc pyrithione shampoo as a face wash daily was initiated. After four weeks of uninterrupted therapy, the patient reported a significant improvement in lesion appearance and reductions in scaling, erythema, pruritus, and burning (Figure 2).
Discussion
Although the etiology of SD is unclear, the skin commensal yeast, Malassezia, and its proinflammatory metabolites have been implicated.2 Topical antifungal treatments have been shown to produce significant decreases in the cutaneous yeast population, correlating with marked visible and symptomatic improvements in SD.3 Topical therapy is generally effective and well tolerated. First-line therapies include topical corticosteroids and antifungals in various vehicles.4 Topical corticosteroids have been shown to be an effective treatment for SD independent of steroid potency.5 Other therapies include calcineurin inhibitors and lithium salts.
The clinical presentation of this patient placed cutaneous sarcoidosis, discoid cutaneous lupus erythematosus, and SD at the top of the differential diagnoses. Cutaneous sarcoidosis, seen in 9 to 37 percent of patients with sarcoidosis and a potential presenting sign of systemic disease, is often characterized by facial non-scaly, mildly symptomatic papules that might coalesce into annular or non-annular plaques.6–9 Although her skin type, clinical distribution, lesion appearance, and past failure to improve with topical medications favored cutaneous sarcoidosis in our patient, the associated scaling and symptoms favored SD.
Conclusion
Progressive facial papules mimicking cutaneous sarcoidosis is a unique–but likely underreported–treatment-responsive variant of SD that might be more likely to be encountered in African-American patients.
Acknowledgments
We thank Julie Jackson, MD, at Westlake Dermatology & Cosmetic Surgery in Austin, Texas, for her role in obtaining a histopathologic diagnosis and Alde Carlo P. Gavino, MD, at Seton Medical Center at the University of Texas in Austin, Texas, for performing histopathologic imaging. Full consent for use of before and after photographs was provided by the patient.
References
- Fritsch PO, Reider N. Other eczematous eruptions. In: Bolgona JL, Jorizzo JL. Rapini RP. Dermatology. 3rd ed. New York, NY: Saunders Elsevier Inc. 2012:219–231.
- Stefanaki I, Katsambas A. Therapeutic update on seborrheic dermatitis. Skin Ther Lett. 2010;15:1–4.
- Kim GK. Seborrheic dermatitis and Malassezia species: How are they related? J Clin Aesthet Dermatol. 2009;2:14–17.
- Shin H, Kwon OS, Won CH, et al. Clinical efficacies of topical agents for the treatment of seborrheic dermatitis of the scalp: a comparative study. J Dermatol. 2009;36:131–137.
- Kastarinen H, Oksanen T, Okokon EO, et al. Topical anti-inflammatory agents for seborrhoeic dermatitis of the face or scalp. Cochrane Database Syst Rev. 2014;5:CD009446.
- Mañá J, Marcoval J. Skin manifestations of sarcoidosis. Presse Med. 2012;41:e355–374.
- Katta R. Cutaneous sarcoidosis: a dermatologic masquerader. Am Fam Physician. 2002;65:1581–1584.
- Mañá J, Marcoval J, Rubio M, et al. Granulomatous cutaneous sarcoidosis: diagnosis, relationship to systemic disease, prognosis and treatment. Sarcoidosis Vasc Diffuse Lung Dis. 2013;30:268–281.
- Callen JP. Sarcoidosis. In: Callen JP, Jorizzo JL, Greer KE, et al. Dermatological Signs of Internal Disease. 4th ed. Philadelphia, PA: Saunders Elsevier Inc, 1995:287–295.