 by Yates Y.Y. Chao, MD; Chiranjiv Chhabra, MBBS, DVD; Niamh Corduff, MBBS, FRACS; Sabrina Guillen FABI, MD; Martina Kerscher, MD; Stephanie C.K. Lam, MBChB; Tatjana Pavicic, MD; Berthold Rzany, MD, ScM; Peter H.L. Peng, MD; Atchima Suwanchinda, MD; Fang-Wen Tseng, MD; and Kyle K. Seo, MD, PhD
by Yates Y.Y. Chao, MD; Chiranjiv Chhabra, MBBS, DVD; Niamh Corduff, MBBS, FRACS; Sabrina Guillen FABI, MD; Martina Kerscher, MD; Stephanie C.K. Lam, MBChB; Tatjana Pavicic, MD; Berthold Rzany, MD, ScM; Peter H.L. Peng, MD; Atchima Suwanchinda, MD; Fang-Wen Tseng, MD; and Kyle K. Seo, MD, PhD
Dr. Chao is with Chao and Chiu Institute of Dermatology, Taipei, Taiwan; Dr. Chhabra is with Skin Alive Clinic, New Delhi, India; Dr. Corduff is with Cosmetic Refinement Clinic, Geelong, Australia; Dr. Fabi is with Cosmetic Laser Dermatology, San Diego, California, USA; Dr. Kerscher is with University of Hamburg, Hamburg, Germany; Dr. Lam is with Central Health Medical Practice, Hong Kong; Dr. Pavicic is in Private Practice for Dermatology and Aesthetics, Munich, Germany; Dr. Rzany is with RZANY & HUND, Berlin, Germany; Dr. Peng is with P-Skin Professional Clinic, Kaohsiung, Taiwan; Dr. Suwanchinda is with Medisci Biointegrative and Antiaging and Cosmetic Medical Center, Bangkok, Thailand; Dr. Tseng is with Milano Aesthetic Clinic, Taipei, Taiwan; and Dr. Seo is with Seoul National University College of Medicine and Modelo Clinic, Seoul, Korea.
J Clin Aesthet Dermatol. 2017;10(7):16–27
Funding: No funding was provided for this study.
Disclosures: Drs. Kerscher, Lam, Peng, Suwanchinda, and Tseng have no conflicts of interest relevant to the contents of this article. Dr. Rzany is a speaker and/or advisor for IPSEN and its affiliates, Galderma and Merz. Dr. Chhabra has no conflicts to disclose. Dr. Seo is a clinical investigator and/or consultant for Allergan, Merz Pharmaceuticals, Q-Med/Galderma, Medytox, LG Life Sciences, and Daewoong. Dr. Corduff is a speaker/advisor for Merz, Motiva, and Spiran. Dr. Fabi is a speaker, consultant, and investigator for Galderma, Merz, Allergan, and Valeant and is an investigator for Revance. Dr. Pavicic is a speaker and/or advisor for Merz, Galderma, Cynosure, Eucerin, Dermaceutic, and Ipsen. Dr. Chao is a speaker and/or advisor for Galderma, Merz, and Valeant.
Keywords: Asian, consensus guidelines, combination treatment, fillers, botulinum toxin
Abstract: Background. The demand for minimally invasive aesthetic procedures has driven requests by physicians for guidance on their use in Asian patients, who have unique cultural preferences, social trends, and anatomy. However, few guidelines exist, particularly on combination treatment strategies for different facial shapes or indications such as the modification of face shapes to the “oval ideal.” Physicians must, therefore, apply Caucasian patient-optimized guidelines to their Asian patients.
Methods. Eleven specialists developed a consensus on the use of botulinum toxin A (BoNT-A), calcium hydroxylapatite (CaHA) and hyaluronic acid (HA) fillers, and microfocused ultrasound with visualization (MFU-V) devices in Asian patients on upper-, middle-, and lower-face indications, including strategies to modify different facial shapes to the oval shape. Approval from 70 to 90 percent of all participants led to moderate consensus, while 90 percent agreement denoted a strong consensus.
Results. For early intervention/enhancement and restoration, most combination strategies are similar between Asian and Caucasian patients. Compared to Caucasian patients, however, beautification is a more common focus in Asian patients. The “ideal” oval facial shape can be created using different interventions depending on the patient’s baseline characteristics.
Conclusions. Although treatments and treatment sequences for early intervention/ enhancement and restoration for beautification in Asian patients are similar to those in Caucasian patients, different treatment strategies may be required.
Introduction
In order for physicians to efficiently deliver optimal patient outcomes, contemporary aesthetic medicine now requires the harmonious combination of multiple aesthetic therapies. Current guidelines with instructive recommendations on the application of combination treatments focus predominantly on Caucasian patients.[1–3] Few such guidelines are available for Asian patients; therefore, physicians must apply recommendations optimized for Caucasian anatomies and aesthetic goals to Asian patients. Asian patients seek aesthetic intervention at a younger age, compared to Caucasians,[4] and their requests typically focus on early intervention/ enhancement, beautification,[5] and the correction of facial deficits.[6] In comparison, Caucasian patients typically seek restorative interventions for more severe, age-related problems. Physicians are inevitably faced with the challenge of effectively adapting nonoptimal treatment recommendations to Asian patients with very different physical presentations, issues, and expectations. This consensus aims to provide much-needed recommendations on aesthetic interventions and combination treatment algorithms for Asian patients, with a particular focus on the application of botulinum toxin A (BoNT-A), injectable fillers, and microfocused ultrasound with visualization (MFU-V). In order for physicians to efficiently deliver optimal patient outcomes, contemporary aesthetic medicine now requires the harmonious combination of multiple aesthetic therapies. Current guidelines with instructive recommendations on the application of combination treatments focus predominantly on Caucasian patients.[1–3] Few such guidelines are available for Asian patients; therefore, physicians must apply recommendations optimized for Caucasian anatomies and aesthetic goals to Asian patients. Asian patients seek aesthetic intervention at a younger age, compared to Caucasians,[4] and their requests typically focus on early intervention/ enhancement, beautification,[5] and the correction of facial deficits.[6] In comparison, Caucasian patients typically seek restorative interventions for more severe, age-related problems. Physicians are inevitably faced with the challenge of effectively adapting nonoptimal treatment recommendations to Asian patients with very different physical presentations, issues, and expectations. This consensus aims to provide much-needed recommendations on aesthetic interventions and combination treatment algorithms for Asian patients, with a particular focus on the application of botulinum toxin A (BoNT-A), injectable fillers, and microfocused ultrasound with visualization (MFU-V).
Consensus Methodology
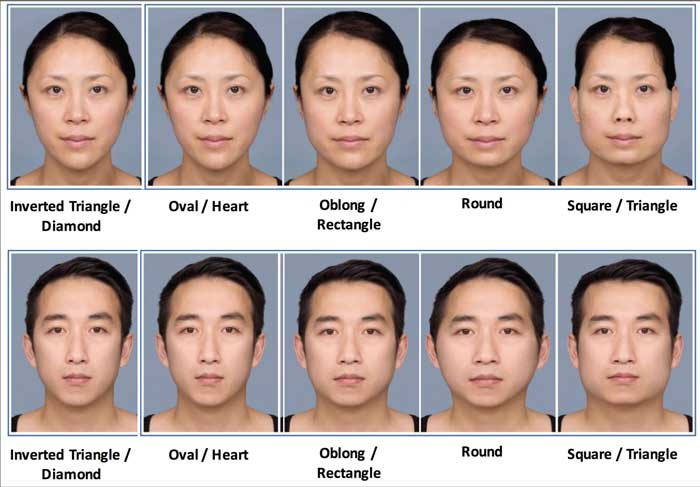
Eleven physicians (“experts”) with experience in treating Asian patients were guided by a certified moderator to discuss combination therapy in Asian populations. The experts voted on recommendations for early intervention/ enhancement, restoration, and beautification and sought to achieve consensus on combination treatment strategies for the modification of different facial shapes (oval/heart, oblong/rectangular, round, square) to the ideal oval shape (Figure 1). Signed patient consent to publish all photos included in this article was obtained by the authors.
The recommendations focused on therapy combining BoNT-A (incobotulinumtoxinA, Xeomin®, Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany), calcium hydroxylapatite (CaHA, Radiesse®, Merz North America, Inc., Raleigh, North Carolina, United States), hyaluronic acid fillers (HA, Belotero® Intense, marketed as Fortélis Extra in Taiwan, and Belotero® Soft, marketed as Esthélis Soft in Taiwan; manufactured by Anteis S.A., Geneva, Switzerland, a wholly owned subsidiary of Merz Pharmaceuticals GmbH, Frankfurt, Germany), and MFU-V (Ultherapy®, Ulthera Inc., Mesa, Arizona, United States).
The experts were from Hong Kong, Taiwan, South Korea, Thailand, India, Australia, Germany, and the United States, and had several years of working experience with all interventions (BoNT-A: average 4.8 years, range 1–10 years; HA: average 4.1 years, range 0.5–10 years; CaHA: average 5.3 years, range 1–8 years; MFU-V devices: average 2.5 years, range 0.5–5 years).
Before the meeting, the experts completed a survey of their clinical experiences with these products to align their knowledge and focus subsequent discussions. Knowledge from a recently published consensus on combined methods in Caucasian patients directed the formulation of recommendations discussed in this document.[1]
 The experts first stated whether they agreed or disagreed with a recommendation. They then discussed their relevant personal clinical experiences and their survey responses. Experts without experience with a technology or topic in Asian patients abstained from voting. Any recommendation failing to achieve a strong or absolute consensus (agreement) was revised or refined, and voting was repeated. Agreement by all experts resulted in an absolute consensus (100%). A “strong” consensus required a minimum of 90-percent agreement or approval, “moderate” consensus required 70- to 90-percent agreement or approval, and “weak” consensus required 50- to 70-percent agreement or approval (Table 1).[7] Two types of wording guided the voting process: “recommend” in cases where data were available and the level of consent was high or “suggest” when personal clinical experience led to a different perspective or less agreement.
The experts first stated whether they agreed or disagreed with a recommendation. They then discussed their relevant personal clinical experiences and their survey responses. Experts without experience with a technology or topic in Asian patients abstained from voting. Any recommendation failing to achieve a strong or absolute consensus (agreement) was revised or refined, and voting was repeated. Agreement by all experts resulted in an absolute consensus (100%). A “strong” consensus required a minimum of 90-percent agreement or approval, “moderate” consensus required 70- to 90-percent agreement or approval, and “weak” consensus required 50- to 70-percent agreement or approval (Table 1).[7] Two types of wording guided the voting process: “recommend” in cases where data were available and the level of consent was high or “suggest” when personal clinical experience led to a different perspective or less agreement.
For consistency, early intervention/ enhancement were defined as treatments performed for prevention or restoration/rejuvenation and to improve or correct flaws and increase youthful appearance. Beautification interventions were defined as procedures performed for natural beautifying purposes (e.g., to reach the desired oval facial shape).
Results
General recommendations. The experts largely agreed with general recommendations proposed for Asian patients; however, notable minor differences were found (Table 2).
Part 1: Combination treatment strategies for Asian patients— specific indications. Upper face indications. Interventions for upper face features discussed here included forehead volume deficiency with or without brow ptosis, forehead rhytides, lateral canthal lines, glabellar frown lines, temporalis hypertrophy, and hollows.
Forehead volume deficiency without brow ptosis. The experts unanimously agreed with the use of HA filler for early intervention/enhancement and restoration (absolute consensus, Table 3A). Concomitant treatment with BoNT-A for the frontalis and corrugator muscle could also be applied in order to prevent unevenness due to muscular activity. The use of a HA filler with projection capacity was recommended for Asian patients.
Forehead volume deficiency with brow ptosis. Asians may naturally lack brow bone contouring or have age-related drooping of the fat pad beneath the brows; therefore, filling of this area can lift brows and “open” the eyes. However, brow ptosis is not commonly treated in Asia. If present, volume deficiency is treated with HA, while eyebrow lifting is performed with BoNT-A.[8] If only early intervention is required, HA treatment alone may be sufficient. BoNT-A treatment is only considered to be effective for hyperactive depressor muscles. Occasionally, BoNT-A can be combined with energy-based devices to treat hypertonic/hyperkinetic supraciliary muscles. If performed on the same day as MFU-V, BoNT-A should be applied immediately after MFU-V treatment (Table 3B). Filling beneath the brows can be done two weeks prior to MFU-V or immediately after MFU-V if done on the same day.
Forehead rhytides. For early intervention/enhancement, the experts suggested using BoNT-A followed by HA fillers (Table 3C), both of which may be applied within the same treatment session. For restoration, energy devices can be used superficially before BoNT-A and filler. To prevent further weakening of the frontalis or if volume deficiency is visible (with or without ptosis), HA could be applied first. Eyebrow position (whether ptotic) may be naturally lower in Asians and can impact the rhytide.[9] To preserve brow position, low-dose or diluted BoNT-A was suggested for forehead rhytides, particularly if treatments for early intervention/enhancement are sufficient.[10]
Lateral canthal lines. Lateral canthal lines are not usually deep in Asian patients, but in cases of severe volume loss, HA can be combined with BoNT-A treatments. Absolute consensus was reached on the recommendations to use only BoNT-A for early intervention and BoNT-A followed by MFU-V and/or HA fillers (to treat loose skin) for restoration.
Glabellar frown lines. While BoNT-A treatment was only suggested for early intervention/enhancement, BoNT-A treatment for restoration received a unanimous recommendation (Table 3E). The experts agreed that restoration should begin with a series of BoNT-A treatments, and, if no sufficient improvement is observed, HA fillers should then be carefully injected into the superficial dermis.
Temporal hollowing and temporalis hypertrophy. Temple hollowing in Asian patients requires more contouring than in Caucasian patients. [11] For early intervention/enhancement of temporal hollows, low doses of HA filler were recommended. For beautification, the combination of HA and/or CaHA was recommended (Table 3F). For temporalis hypertrophy, BoNT-A rather than fillers was recommended for all aesthetic goals (Table 3G).
Mid-face indications. Mid-face indications discussed included nose shaping, cheek volume, and nasolabial folds (Table 4).
Cheek volume deficiency (anteromedial, submalar, and subzygomatic). Weak consensus was given for the use of MFU-V first to reposition superficial fat pads as an early intervention/ enhancement in the treatment of cheek volume deficiencies that were not affected by laxity (Table 4B). To address volume loss, fillers (HA or CaHA) were suggested (Table 4A–C) for early intervention/enhancement. For cheeks suffering laxity, MFU-V treatment immediately before HA and/or CaHA fillers was suggested for same-day restoration treatments, as published in previous consensus statements.[1] For early combination interventions, MFU-V (to tighten skin) and/or HA (to volumize) treatments were suggested. As CaHA filler has volumization and skin-tightening benefits, it can be used alone to treat skin laxity or in combination with MFU-V. HA and/or CaHA fillers were recommended for anteromedial, submalar, and subzygomatic cheek areas; however, only advanced users should attempt CaHA fillers in the anteromedial cheek (Table 4A–C).
Nose shaping. The use of HA fillers and/or CaHA before BoNT-A (if indicated; Table 4D) was recommended for nose shaping, which was considered a beautification procedure rather than an early intervention/ enhancement or restoration intervention. The high risk of vascular compromise in this area requires that interventions involving CaHA be performed only by skilled injectors.
Nasolabial fold (NLF). The NLF was differentiated into upper and lower folds due to the potential for vascular compromise.[12] Correction through lateral facial revolumization should always be attempted first. For the upper fold, only HA fillers for early intervention/enhancement and HA fillers and/or CaHA fillers for restoration (Table 4E) were recommended.
Lower-face indications. Lower-face indications discussed included perioral rhytides, lip fullness, marionette lines, chin, mental crease, and jawline (Table 5).
Perioral rhytides. The use of BoNT-A before HA fillers for early intervention/enhancement and BoNT-A with HA fillers before MFU-V for the restoration of perioral rhytides (Table 5A) were recommended. Readers are urged to refer to the previous consensus publication for recommended treatment timeline.[1] Several experts suggested using BoNT-A only for early intervention/ enhancement or if “mimetic activity” was pronounced.
Lip fullness/enhancement. Lip enhancement or shape change would be considered a beautification procedure in patients with sufficient lip volume (Table 5B). While CaHA is contraindicated for this indication, HA is recommended.
Marionette lines. While some experts agreed that early intervention/enhancement required BoNT-A, others suggested using MFU-V to minimize jowl fat pad protrusion or combining BoNT-A with fillers for restoration. HA and/or CaHA should be applied over the prejowl sulcus following mid-face restoration interventions (Table 5C).
Mentalis. BoNT-A may be utilized only if mimetic activity was observed, and first line treatment with toxin was recommended for early intervention/enhancement and restoration (Table 5E).
Jawline. CaHA, high in elasticity and viscosity, is ideal for jawline creation. For beautification, the masseter or platysma, but not the jaw, should be treated with toxin, while filler should be used to sculpt different shapes and increase bone definition (Table 5F).
Masseter hypertrophy. The use of BoNT-A for all interventions was recommended (Table 5G). Toxin dose is a critical consideration.[13,14] Toxin denervation without concomitant prejowl/chin augmentation can result in jowl fat sagging; hence, combination treatments are recommended. For early intervention/enhancement and beautification, most patients may require only BoNT-A for the masseter. However, older patients with prominent jowls and submalar and subzygoma depressions may require concurrent filler augmentation of the cheek and chin or MFU-V for lifting.
Part 2: Combination treatment strategies for Asian patients— Modifying face shapes to achieve the “oval ideal.” The experts unanimously agreed that the oval or heart facial shape was an aesthetic goal of Asian patients and that combination treatments were recommended to achieve this because single interventions were unlikely to produce significant changes. This consensus focused on the treatments and treatment sequences, as these may be influenced by patient factors, such as cultural preferences and personal finances.
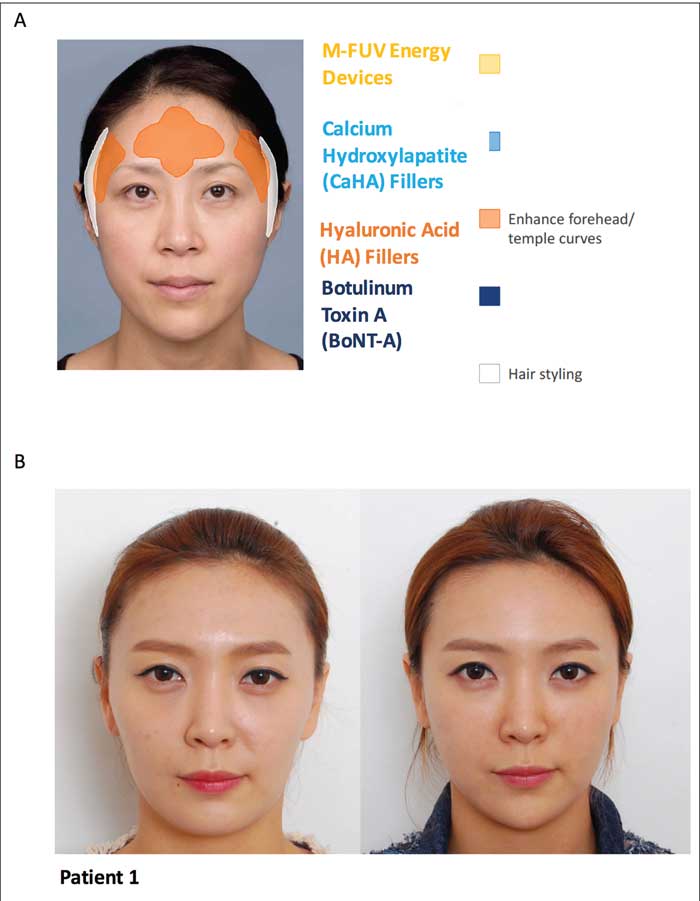
Treatment suggestions for patients with the ideal oval/heart face shape. For beautification or enhancement of facial features that are less prominent in Asians, only specific concerns should be addressed. For example, filler can be injected into the medial cheek or pyriform aperture for anterior projection of the nose or concavities. For more heart-shaped faces, augmentation of the medial malar area may be necessary for oval shaping and to increase anterior projection (Figure 2).
Treatment suggestions for patients with oblong/rectangular face shape. Oblong/rectangular faces contain a longer mandibular bone that pulls fat downward and flattens the central area. This requires lower face narrowing and smoothing, midface/anterior area projection, temple and forehead smoothing, and nose and lip augmentation (Figure 3).

Treatment suggestions for patients with round face shape. To bring the round face closer to the oval shape, the masseter should be reshaped and contoured via BoNT-A injection to slim or narrow the lower face, and midface anterior projection should be improved through chin elongation (Figure 4).
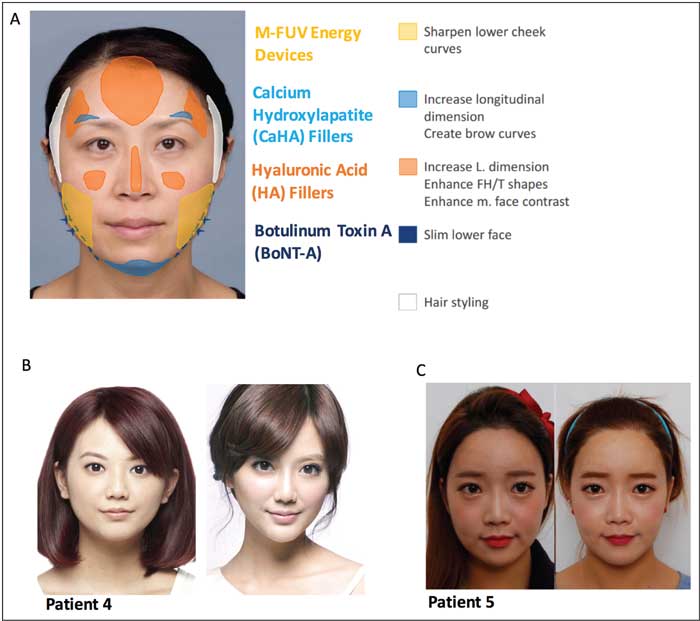
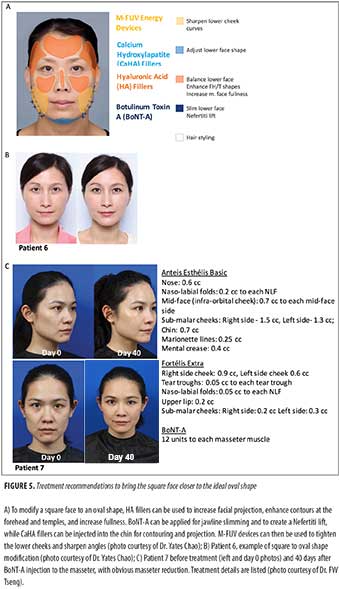
Treatment suggestions for patients with square face shape. Due to the magnitude of corrections required, square faces need the most interventions (Figure 5).
Discussion
The experts agreed that cultural and country-specific preferences determine aesthetic goals and must be included as part of aesthetic treatment strategies.
East Asians do not generally find square, thin faces attractive but prefer softer, more oval-shaped faces for both sexes.[15–17] While similarities do exist and can be applied to all Asian nationalities, some critical differences in preferences are apparent, especially in what is considered congenital and what is considered aesthetically appealing. Korean faces, for example, have fuller, chubbier cheeks with shorter faces,[17] while Chinese faces have relatively narrow, slim faces with longer jaws, fuller lips, and narrower noses.[18,19]
In the treatment of Korean women for forehead volume deficiencies with brow ptosis, overly arched or lifted brows and lateral orbital rims must be avoided, as these are perceived as exaggerated and aggressive.[20,21] Physicians, therefore, use MFU-V treatments for brow ptosis in these patients. Chinese patients often request filler augmentation in the temporal area, regardless of whether they have significant temporal hollowing and temporalis hypertrophy, as the area is thought to represent fortune in Chinese culture.
Treatment recommendations for the NLF vary among Asian countries. Some physicians consider the upper NLF to be a natural curve rather than a flaw and will avoid overtreatment here, whereas others use MFU-V and inverse contraction of the nasolabial fat pad to lift the midface area. To treat masseter hypertrophy, Taiwanese physicians address the entire face rather than just the affected area, while Thai physicians use a lower dose of BoNT-A for masseter restoration alongside other interventions for excessive sagging.
Some aesthetic preference commonalities exist. For example, due to unattractive or extreme images in the media, Asian patients refrain from lip plumping interventions. Asian chins tend to be smaller and recessed,[22,23] resulting in age-related and congenital deficiencies. Therefore, unlike Caucasians, Asians seek treatment for chin volume loss, rather than for chin projection.[24] Most Korean patients find longer faces unappealing.[25] Thus, while small-chin volumization requires fillers, Korean physicians do not usually perform chin volume augmentation.
Aging-related bone recession and fat pad atrophy also affect treatment strategy.[26] Elderly patients may display chin irregularities caused by the mentalis muscle contracting onto atrophied bone. If this volume loss is age-related, the mentalis muscle will contract into this void[27] and require combination treatment. Age-related subzygomatic volume deficiency and atrophy[28] necessitate concurrent restorative interventions. Interestingly, subzygomatic depressions unrelated to laxity are frequently treated in young, East Asian women, together with oval-face shaping and a reduction of subzygomatic prominence.[29,30]
Sex-determined goals also exist, particularly for beautification of the jawline. Asian men prefer straight, defined jaws but not broad or square jaws (in contrast to Caucasians).[31] Jawline reduction and definition are frequently requested by Asian women;[32] mandibular angle augmentation is smore common than toxin treatment in Korea.[33,34] To create a more defined jawline in Taiwanese men, MFU-V, toxin, and filler treatments are administered, as toxin alone is ineffective. These distinctions suggest that Taiwanese and Korean patients have different aesthetic goals for the jawline (Table 5F).
Conclusion and Future Directions
To our knowledge, this is the first description of the aesthetic treatments required to achieve facial changes considered “ideal” for the Asian patient. It is not our intention to provide detailed treatment instructions, which can be found elsewhere.1
Our current recommendations for combined interventions in Asian patients complement previous work1,35 by providing granular recommendations for early intervention/enhancement, restoration, or beautification treatments in Asians.
The experts in this current consensus displayed a high level of agreement with World Congress of Dermatology Consensus statements, demonstrating that the goals of beautification and treatment strategies using minimally invasive technologies are actually similar between Caucasian and Asian patients. However, the indications, filler types, and dosages of botulinum toxin are factors that must be customized to the specificities of Asian faces.
The recognition and understanding of facial shapes is near universal but often focuses on the oval facial shape.[36–39] In reality, ethnicity and societal preferences influence patient preferences.[40] Therefore, this consensus provides some guidance on the procedures necessary for the modification of nonideal face shapes to the oval ideal in individual patients. Combination treatments should be used holistically to reduce widths, angularity, and masculine features and to enhance feminization, three-dimensional projection, and contours in women. Ethnicity-determined congenital deficiencies and cultural biases should be respected and carefully considered during patient selection, counselling, and the formulation of optimal treatment plans. For the first time, this document establishes consensus recommendations and clinical guidance for physicians who wish to treat Asian patients more effectively and with optimal outcomes using defined combined interventions.
References
- Carruthers J, Burgess C, Day D, et al. Consensus recommendations for combined aesthetic interventions in the face using botulinum toxin, fillers, and energy-based devices. Dermatol Surg. 2016;42(5):586–597.
- Sundaram H, Liew S, Signorini M, et al. Global Aesthetics Consensus Group. Global aesthetics consensus: hyaluronic acid fillers and botulinum toxin type A-recommendations for combined treatment and optimizing outcomes in diverse patient populations. Plast Reconstr Surg. 2016;137(5):1410–1423.
- Wu WT, Liew S, Chan HH, et al. Asian Facial Aesthetics Expert Consensus Group. Consensus on current injectable treatment strategies in the Asian face. Aesthetic Plast Surg. 2016;40(2):202–214.
- Liew S, Wu WT, Chan HH, et al. Consensus on changing trends, attitudes, and concepts of Asian beauty. Aesthetic Plast Surg. 2015 Sep 25. [Epub ahead of print]
- Weng CJ. Oriental upper blepharoplasty. Semin Plast Surg. 2009;23(1):5–15.
- Liew S. Ethnic and gender considerations in the use of facial injectables: Asian patients. Plast Reconstr Surg. 2015;136(5 Suppl):22S–27S.
- German Association of the Scientific Medical Societies (AWMF)— Standing Guidelines Commission. AWMF Guidance Manual and Rules for Guideline Development, 1st ed. 2012. English version. http://www.awmf.org/fileadmin/user_upload/Leitlinien/AWMF-Regelwerk/AWMF-Guidance_2013.pdf. Accessed November 26, 2015.
- Young SM, Lim LH, Seah LL, et al. Prospective audit of ptosis surgery at the Singapore National Eye Centre: two-year results. Ophthal Plast Reconstr Surg. 2013;29(6):446–453.
- Rhee SC, Woo KS, Kwon B. Biometric study of eyelid shape and dimensions of different races with references to beauty. Aesthetic Plast Surg. 2012;36(5):1236–1245.
- Wu WT. Microbotox of the lower face and neck: evolution of a personal technique and its clinical effects. Plast Reconstr Surg. 2015;136(5 Suppl):92S–100S.
- Watanabe K, Miyagi H, Tsurukiri K. Augmentation of temporal area by insertion of silicone plate under the temporal fascia. Ann Plast Surg. 1984;13(4):309–319.
- Beleznay K, Humphrey S, Carruthers JD, Carruthers A. Vascular compromise from soft tissue augmentation: experience with 12 cases and recommendations for optimal outcomes. J Clin Aesthet Dermatol. 2014;7(9):37–43.
- Ganceviciene R, Liakou AI, Theodoridis A, et al. Skin anti-aging strategies. Dermatoendocrinol. 2012;4(3):308–319.
- Ahn KY, Park MY, Park DH, Han DG. Botulinum toxin A for the treatment of facial hyperkinetic wrinkle lines in Koreans. Plast Reconstr Surg. 2000;105(2):778–784.
- Li X, Hsu Y, Hu J, et al. Comprehensive consideration and design for treatment of square face. J Oral Maxillofac Surg. 2013;71(10):1761.e1–14.
- Mu X. Experience in East Asian facial recontouring: reduction malarplasty and mandibular reshaping. Arch Facial Plast Surg. 2010;12(4):222–229.
- Lee JS, Kim HK, Kim YW. Anthropometric analysis of the attractive and normal faces in Korean female. J Korean Soc Plast Reconstr Surg. 2004;31(4):526–531.
- Zhao Q, Zhou R, Zhang X, et al. Morphological quantitative criteria and aesthetic evaluation of eight female Han face types. Aesthetic Plast Surg. 2013;37(2):445–453.
- Wu F, Li J, He H, et al. Soft-tissue facial characteristics of attractive Chinese men compared to normal men. Int J Clin Exp Med. 2015;8(5):7977–7982.
- Kim BW, Park GH, Yun WJ, et al. Adverse events associated with botulinum toxin injection: a multidepartment, retrospective study of 5310 treatments administered to 1819 patients. J Dermatolog Treat. 2014;25(4):331–336.
- Lam SM. Aesthetic strategies for the aging Asian face. Facial Plast Surg Clin North Am. 2007;15(3):283–291.
- Shirakabe Y, Suzuki Y, Lam SM. A new paradigm for the aging Asian face. Aesthetic Plast Surg. 2003;27(5):397–402.
- Hwang WS, Hur MS, Hu KS, et al. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. Angle Orthod. 2009;79(1):70–77.
- Lee TS, Kim HY, Kim TH, et al. Contouring of the lower face by a novel method of narrowing and lengthening genioplasty. Plast Reconstr Surg. 2014;133(3):274e–282e.
- Kim TG, Lee JH, Cho YK. Inverted V-shape osteotomy with central strip resection: a simultaneous narrowing and vertical reduction genioplasty. Plast Reconstr Surg Glob Open. 2014;2(10):e227.
- Coleman SR, Grover R. The anatomy of the aging face: volume loss and changes in 3-dimensional topography. Aesthet Surg J. 2006;26(1S):S4–9.
- Rohrich RJ, Pessa JE. The anatomy and clinical implications of perioral submuscular fat. Plast Reconstr Surg. 2009;124(1):266–271.
- Buckingham ED, Glasgold R, Kontis T, et al. Volume management of the middle third-lower orbit/midface. Facial Plast Surg. 2015;31(1):55–69.
- Lee HY, Yang HJ, Cho YN. Minimally invasive zygoma reduction. Plast Reconstr Surg. 2006;117(6):1972–1979.
- Lee JG, Park YW. Intraoral approach for reduction malarplasty: a simple method. Plast Reconstr Surg. 2003;111(1):453–460.
- Lee HY, Yang HJ, Cho YN. Minimally invasive mandible reduction using Lee’s Rasp & Saw. Aesthetic Plast Surg. 2007;31(2):201–205.
- Lee TS, Kim HY, Kim T, et al. Importance of the chin in achieving a feminine lower face: narrowing the chin by the “mini V-line” surgery. J Craniofac Surg. 2014;25(6):2180–2183.
- Kim NH, Chung JH, Park RH, Park JB. The use of botulinum toxin type A in aesthetic mandibular contouring. Plast Reconstr Surg. 2005;115(3):919–930.
- Jin H. Misconceptions about mandible reduction procedures. Aesthetic Plast Surg. 2005;29(4):317–324.
- Rho NK, Chang YY, Chao YY, et al. Consensus recommendations for optimal augmentation of the Asian face with hyaluronic acid and calcium hydroxylapatite fillers. Plast Reconstr Surg. 2015;136(5):940–956.
- Farhadian JA, Bloom BS, Brauer JA. Male aesthetics: a review of facial anatomy and pertinent clinical implications. J Drugs Dermatol. 2015;14(9):1029–1034.
- Li J, Hsu Y, Khadka A, et al. Contouring of a square jaw on a short face by narrowing and sliding genioplasty combined with mandibular outer cortex ostectomy in orientals. Plast Reconstr Surg. 2011;127(5):2083–2092.
- Mitteroecker P, Windhager S, Müller GB, Schaefer K. The morphometrics of “masculinity” in human faces. PLoS One. 2015;10(2):e0118374.
- Pedrosa VO, França FM, Flório FM, Basting RT. Study of the morpho-dimensional relationship between the maxillary central incisors and the face. Braz Oral Res. 2011;25(3):210–216.
- Li D, Xu H, Xu L, et al. The aesthetic proportion index of facial contour surgery. J Craniofac Surg. 2015;26(2):586–589.